Our Top Story: America Trains Enough Doctors — Redefining Medical Supply and Demand
(Edited from KevinMD post by dermatology practice co-founder Rushi Negalla)
If the US medical system is a chessboard, and providers are the game pieces, America is playing those pieces with one column, row, and role instead of using the whole space.
Several journals, economists and medical professionals forecast physician supply to be dangerously low in 10- to 20-plus years. They’re 100% correct that supply won’t meet demand (as things stand now), but the reasons are flawed.
Alarmists have been complaining about doctor shortages for decades. Physician retirement and burnout don’t explain predicted gaps. The physician shortage everyone worries about is not a lack of new graduates but a grand misallocation of resources.
[Editor’s Note: While the debate continues–and until physician supply is increased or reallocated rather dramatically–the outlook for the locum tenens industry remains bright.]
The Numbers Don’t Tell All
In terms of raw supply, there are just over one million licensed physicians. According to a Federation of State Medical Boards census, the number of doctors grew by 20% from 2010 to 2020. Most of that growth (+168K physicians) is from new graduates.
In the same period, the US population rose ~7% to ~330M. The seemingly reassuring headline numbers are misleading.
In terms of fresh supply, the number of medical school graduates rose by 32% between 2011 to 2021, but in absolute terms, there were ~28K grads last year. The US population is a slow-growing mega-fountain, while medical providers are a fast-flowing sink faucet. It’s not practical to expect both to balance each other without help.
Shortage and Supply Aren’t the Same
More data gathered by the Kaiser Family Foundation indicate that one primary care doctor serves 665 people on average, while one specialist serves 584 people. The doctor-to-patient ratios appear extremely low in a vacuum, but most physicians can handle patient groups in the low thousands. There’s a critical difference between real capacity and max capacity.
If the US population doubled tomorrow, one average PCP could oversee ~1,300 patients, and one specialist ~1,100 patients. So why do both patients and economists keep worrying about doctor capacity? The answer: Shortage isn’t the same as supply.
Physicians don’t magically pop into clinics, see patients, and then poof away. Amazon.com is better at delivering packages anywhere in two days than we are at having doctors in the right place at the right time.
Hyper-urbanized regions have too many doctors chasing relatively concentrated patient populations. Meanwhile, rural areas have too few doctors to care for smaller numbers of patients who are more widely dispersed.
Most physicians in private and public settings practice during the traditional workweek, some limiting their patient appointments to just a few weekdays. Physicians have to do paperwork alongside patient care.
Even if physicians make themselves available to see thousands of people each, those doctors may still reject Medicare and Medicaid patients because such plans typically reimburse at much lower rates than private insurers do.
To remedy some of these healthcare-delivery woes, our physician supply needs to be realigned instead of rebuilt.
Realign, Rather Than Rebuild
Expanding AI office solutions, targeting more patient demographics by redefining “availability,” and carefully expanding the non-physician workforce (e.g., nurse practitioners and physician assistants) can maximize each doctor’s max patient panel enough to keep up with demand.
Fine-tuning office-visit timing while embracing technology and easing administrative hassles (i.e., vertically integrated disease/drug literature banks, chart notes, insurance claims, and payment systems) are the most appropriate supply-side adjustments. Offering additional time over weekends or after normal business makes care accessible to patients in certain demographies.
Supply must reach demand somewhere. Our country’s true medical care needs create the shortage in the first place. The Association of American Medical Colleges, or AAMC, publishes a 25-year forecast of physician supply. In their 2019 to 2034 review, the authors calculated demand based on demographic changes, the incidence of diseases affecting the related demographics, and care delivery setting.
Current U.S. medical needs suggest a lack of ~38K to 124K physicians and ~18K to 48K primary care doctors by 2034. Those are massive gaps compared to ~28K expected new medical graduates in 2021, but the AAMC lowered both top ends of those ranges by 12 to 14% year-over-year from their last report. The report highlights four nationwide scenarios for improving real medical capacity (and reducing shortage forecasts).
Total Physician Supply and Demand
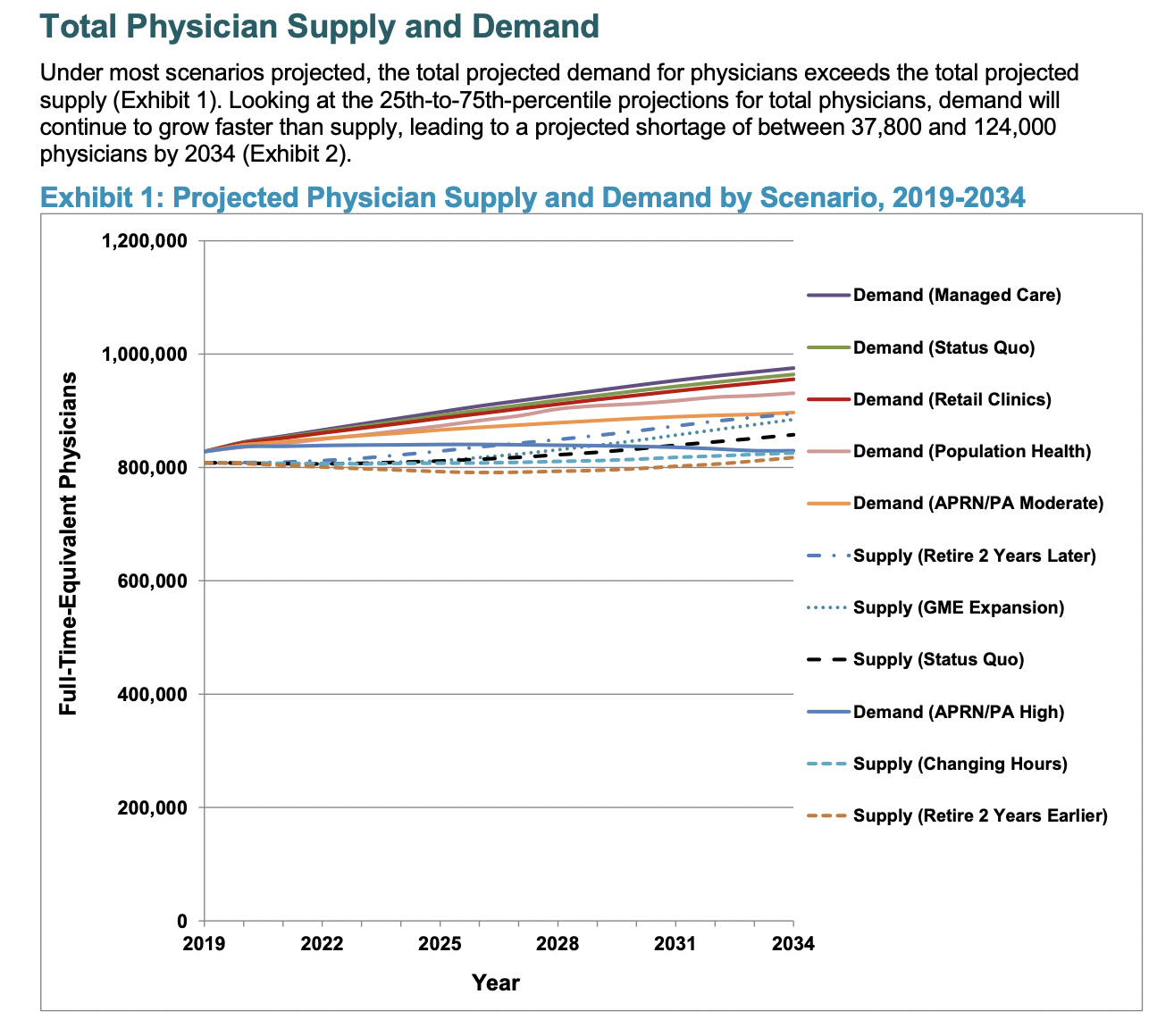
Source: AAMC’s The Complexities of Physician Supply and Demand Report June 2021
Stretching Supply is Easier Than Reducing Demand
The first interesting, but impractical, shift to ease demand would have all covered patients join an HMO or ACO insurance network. In this world, medicine, doctors and money are vertically integrated like a company that owns its whole supply chain.
Unending political gridlock precedes this outcome based on current US healthcare policy and current insurance and physician trade group positioning.
The second demand scenario involves magical thinking, but remains a helpful reference point. The AAMC modeled what might happen if we all lost weight, cut glucose, quit smoking, and reduced cholesterol. Population-wide health improvements prevent shortfalls–but we’re human.
The next two possible futures in extending supply appear somewhat reasonable.
Thinking More Realistically
First, drugstore chains like CVS and Walgreens are sprouting more and more clinics. The proliferation of these retail clinics introduces alternative primary care facilities treating minor, but acute, issues. It’s efficient for patients to get basic goods, prescriptions, and routine medical exams at the same place. If referrals are necessary, patients can still get those permissions and move on to see specialists rather than wait for advice from traditional medical practices.
Second, adding more registered nurses and physician assistants under strict oversight could help plug gaps of care that doctors can’t easily reach.
Combining all these scenarios might ensure that providers can heal Americans faster while preventing the need to grow doctors on trees.
Whatever the consensus definition for the US physician shortage, cleaning up healthcare delivery, better utilizing retail clinics and advanced practitioners, and redefining availability to target broader patient-demographic segments can reduce the gap between clinician supply and patient demand. Patients who understand this situation will better handle whatever changes occur next to our fragmented healthcare system.
The late Dr. Ken Teufel quoted Harvard Business Review’s advisory board in a “Dr. Ken’s Corner” blog post for Interim Physicians dated June 23, 2020 [speaking about a predicted deficit of primary care physicians that could grow to 55,000 PCPs by 2023]: “It’s time to stop panicking about a looming ‘shortage.’ Rather, the real shortage is one of courage to disrupt the way things have been done for decades.”
All News Is Locums
7 Ways You Make an Impact as a Locum Tenens Provider
(Edited from All Star Healthcare Solutions® blog, 8/10/2022)
Whether you choose locum tenens to supplement your income, to experience a variety of locations and settings, or to transition into a new career stage (from residency to retirement and in between), you make an important impact with each assignment.
1. You extend high-quality care to those in need.
According to McKinsey research, 45% of Americans admit to having at least one unmet healthcare need. Locum tenens professionals help mitigate those circumstances, so individuals can receive the attention they need and deserve. What’s more, because locum tenens providers are not involved with many of the facility’s administrative duties, you have more freedom to hone in on patient interactions.
2. You empower facilities to maintain continuity of care.
Hospitals, clinics, and other healthcare organizations experience fluctuations in patient census, personnel vacancies or family/medical leaves, and other factors that affect staffing needs. Accepting locum tenens jobs not only answers the demand for clinicians, but also helps facilities preserve continuity of care, too. Units are better manned to meet patient demand and sustain services.
3. You provide specialty coverage.
The shortage of primary care physicians has been well documented; however, numerous specialties remain underrepresented. For example, the American Journal of Surgery published a study that indicates nine surgical specialties are in jeopardy of incurring staffing shortages by 2030. Compounding the situation is a concentration of high-acuity specialists choosing to practice in urban centers, which leaves smaller and rural communities at a disadvantage. Whether your locum tenens contracts take you to the country or a city, as a specialist, you make an impact on patients’ care and a facility’s ability to meet the community’s needs.
4. You ease the demand on staff.
As patient needs grow, so does the call for quality clinicians, even though the physician shortage shows no signs of slowing. This confluence of factors creates a dynamic that weighs heavily on a facility’s personnel—namely, larger caseloads and longer hours. According to a pre-COVID survey conducted by The Physicians Foundation, the majority of physicians average between 41 and 60 hours on the job per week. Locum tenens providers help even out duties by assuming a portion of caseloads. Advanced practice providers in temporary positions also shift clinical responsibilities, allowing physicians to concentrate on more critical cases.

5. You share your skills.
As a locum tenens professional, you are invited to observe various practice styles and how cultural and regional aspects influence healthcare. Accumulating that knowledge can enhance your own practice as well as impact fellow practitioners and their patients by sharing the experiences you collect along the locum tenens journey.
6. You support the community.
Your presence can make a noteworthy difference where access to healthcare infrastructure is limited. For example, the Association of American Medical Colleges (AAMC) confirms three out of five federally designated health professional shortage areas exist in rural areas. Fulfilling locum tenens assignments at rural facilities, or within urban healthcare deserts, expands care for patients but supports the facility’s role in the greater community, too. Hospitals typically operate as a major employer in town and contribute to the local economy. So, even temporarily, your contribution leaves a larger impact on the community in addition to treating individuals.
7. You become a friend.
Yet another impactful impression locum tenens professionals make is with their friendship, forming enduring relationships with co-workers you meet on each opportunity.
Faster Licensing in 32 States And Territories with the Interstate Medical Licensure Compact
(Edited from Global Medical Staffing Blog post by Kari Redfield, 7/13/2022)
Physicians can now get expedited licensure to practice medicine in most US states. The Interstate Medical Licensure Compact (IMLC) allows medical doctors to move quickly through the licensure process in 31 states and the territory of Guam.
This is a boon for physicians interested in working locum tenens. Interested in working in Guam so you can enjoy the tropical climes and experience a new culture? Great! You can get started much more quickly. Want to escape the winter blues for some weekend shifts in sunny Texas? Awesome. Let’s get you lined up.
Getting licensed in additional states is simpler with the ever-expanding number of IMLC-member states. And the IMLC process reduces the time to get a new license from months to just weeks in many cases.
How It Works
As the IMLC explains, eligible doctors complete a single application and then receive separate licenses from each state in which they intend to practice.
As usual, the license is issued by each individual state, but because the application goes through the IMLC the overall process is streamlined. That means that you can get licensed to practice in more states faster and with less work.
So how do you qualify and apply? And how long does it take? Keep reading.
Rather see this all through a video? Watch a general overview here.
How You Qualify
First, you need to declare your “State of Principal License” (SPL), where you hold a full and unrestricted medical license. To designate your SPL, you must complete an application and then receive a formal Letter of Qualification from that state. Then the SPL shares this information with the additional states where you want to practice.
The Interstate Medical Licensure Commission explains the qualifications that are required to apply for a license. At least one of the following must apply:
- Your primary residence is in the SPL.
- At least 25% of your practice of medicine occurs in the SPL.
- You’re employed to practice medicine by a person, business or organization located in the SPL.
- You use the SPL as your state of residence for US federal income tax purposes.
And, of course, you must be in good standing without a criminal history, have no disciplinary actions against your medical license, or be under investigation.
[Watch a video about qualifying for the IMLC here.]
You must:
- Have graduated from an accredited medical school, or a school listed in the International Medical Education Directory.
- Have successfully completed ACGME- or AOA-accredited graduate medical education.
- Passed each component of the USMLE, COMLEX-USA, or equivalent in no more than three attempts for each component.
- Hold a current specialty certification or time-unlimited certification by an ABMS or AOABOS board.
Following these standards, about 80% of US physicians already meet the criteria for licensure through the Compact.
States and Territories that Offer Expedited Licensure
(IMLC-member states map as of March 2022):
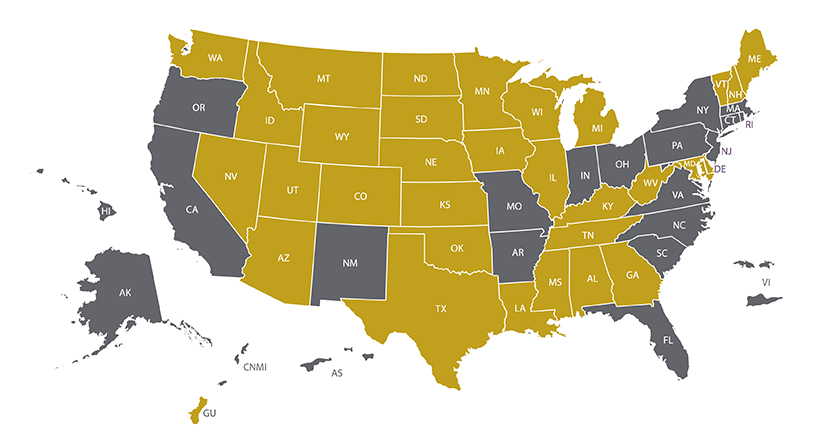
Many states have elected to join the IMLC voluntarily to help address the physician shortage. To participate, a state’s legislature introduces and enacts a bill authorizing the state to join. Current IMLC member states and territories include: